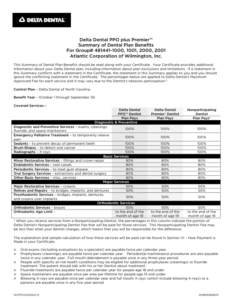
Atlantic Packaging offers a dental program through Delta Dental. The chart below is a brief outline of the plan. Please refer to the summary plan description for complete plan details.
While the coverage is the same in- and out-of-network, you will pay less out of pocket if you visit an in-network provider with Delta Dental.
Diagnostic & Preventive* oral examination, cleaning, all x-rays, topical application of fluoride solution for dependent children up to age 19, space maintainers, sealants for children up to age 16
100%
100%
Basic extractions, fillings, oral surgery, lab services required for procedures, general anesthesia, endodontic and periodontal care
80%
80%
Major crowns, inlays/onlays, bridges, dentures, implants
50%
50%
Orthodontia (covered dependent children up to age 19)
Benefit Percentage
50%
50%
Lifetime Maximum
$1,000
$1,000
*Preventive Incentive – Diagnostic and Preventive Services do not count toward the annual maximum
Delta Dental Benefit Summary
PPO PLUS PREMIER Find a Dentist Flier NORTH CAROLINA