Atlantic Packaging offers two medical plans administered through our Third-Party Administrator, Health Plans, Inc.В
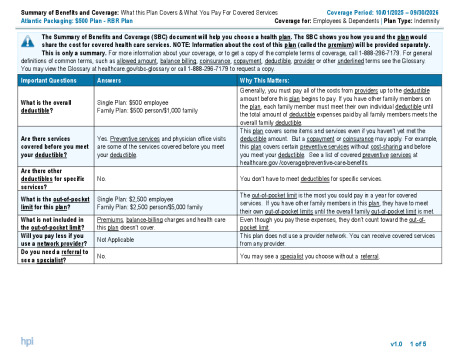
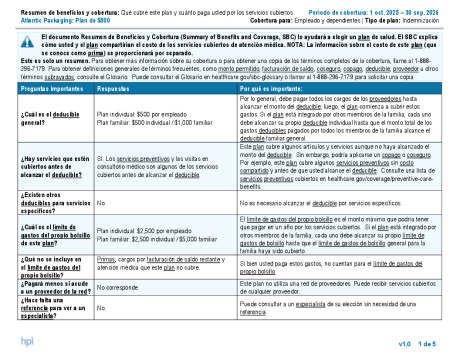
RBR Medical Plan
The RBR Medical Plan will remain unchanged. Preventive care is still covered at 100%, with no copay or out-of-pocket cost. Copays are:В
$25 for primary care visits
$50 for specialist visits
$250 for the first ER visitВ
The annual deductible is $500 per person, and the out-of-pocket maximum is $2,500 per person. That means after you pay the first $500 in covered expenses, you’ll pay 20% of the remaining costs until you hit the $2,500 cap. For families, two members must each meet the $500 deductible and $2,500 out-of-pocket max, totaling $1,000 deductible and $5,000 out-of-pocket max for the family.
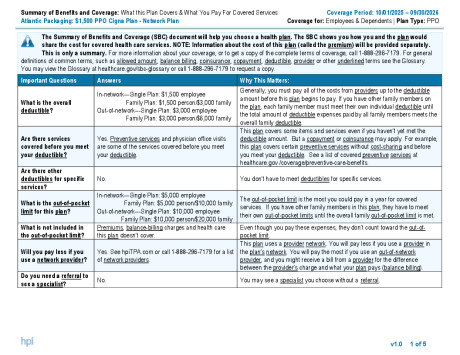
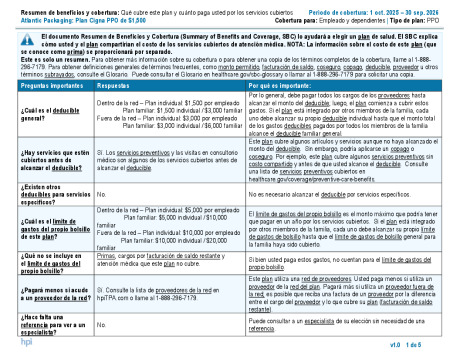
CIGNA Network Medical PlanВ
The Network Medical Plan, offered through HPI and using the CIGNA Network, gives you access to a broader range of providers and covers 98% of our geographic footprint but comes with higher costs due to fewer network discounts. Preventive care is still fully covered, but the rest of the costs are a bit different.В
$35 for primary care visits
$75 for specialist visits
$500 for the first ER visitВ
The annual deductible is $1,500 per person and $3,000 per family, with an out-of-pocket maximum of $5,000 per person and $10,000 per family. Just like the RBR plan, once you meet your deductible, you’ll pay 20% of covered expenses until you hit that out-of-pocket max.
The chart below provides a brief outline of what is offered.В
Cost of Coverage
Employee Contributions
Weekly Employee Contributions
RBR Plan
Network Plan
Standard Rate
Wellness Rate*
Standard Rate
Wellness Rate*
Employee
$43.02
$19.79
$43.02
$19.79
Employee & Spouse
$122.52
$84.54
$122.52
$84.54
Employee & Child(ren)
$93.85
$61.95
$93.85
$61.95
Employee & Family
$221.08
$168.02
$221.08
$168.02
Monthly Employee Contributions
RBR Plan
Network Plan
Standard Rate
Wellness Rate*
Standard Rate
Wellness Rate*
Employee
$186.44
$85.76
$186.44
$85.76
Employee & Spouse
$530.91
$366.33
$530.91
$366.33
Employee & Child(ren)
$406.70
$268.43
$406.70
$268.43
Employee & Family
$958.01
$728.09
$958.01
$728.09
*Wellness premiums are based on program participation
Coverage
Medical Plan Benefits
RBR Plan
Network Plan
Annual Deductible
In-Network
Out of Network
Individual
$500
$1,500
$3,000
Family
$1,000
$3,000
$6,000
Coinsurance
20%
20%
40%
Maximum Out-of-Pocket*
Individual
$2,500
$5,000
$10,000
Family
$5,000
$10,000
$20,000
Physician Office Visit
Primary Care
$25 copay
$35 copay
40% after deductible
Specialty Care
$50 copay
$75 copay
40% after deductible
Teladoc
$0 copay
$0 copay
Not Available
Preventive Care
Adult Periodic Exams
100% Covered
100% Covered
40% after deductible
Well-Child Care
100% Covered
100% Covered
40% after deductible
Diagnostic Services
X-ray and Lab Tests
100% Covered
100% Covered
40% after deductible
Complex Radiology
20% after deductible
20% after deductible
40% after deductible
Urgent Care Facility
$50 copay
$100 copay
40% after deductible
Emergency Room Facility Charges
$250 copay for first visit, then 20% after deductible for subsequent visits
$500 copay for first visit, then 20% after deductible for subsequent visits
Inpatient Facility Charges
20% after Deductible
20% after Deductible
40% after deductible
Outpatient Facility and Surgical Charges
20% after deductible
20% after Deductible
40% after deductible
Mental Health
Inpatient
20% after deductible
20% after Deductible
40% after deductible
Outpatient
$25 copay
$35 copay
40% after deductible
Substance Abuse
Inpatient
20% after deductible
20% after deductible
40% after deductible
Outpatient
$25 copay
$35 copay
40% after deductible
Other Services
Chiropractic
$50 Copay (30 visits combined with other outpatient therapies per plan year)
$75 Copay (30 visits combined with other outpatient therapies per plan year)